Anaesthetic Assessment
This assessment took place on the day of surgery, at this point the plan for the anaesthetic was discussed with George and he was consented for the procedure with the surgeons.
The anaesthetic plan for George was:
Arterial line
Epispinal
General Anaesthetic
Central Line
Consent:
George was consented under a consent form 1 for a Aortobifem bypass + Left Femoral popliteal bypass +/- Fem Fem crossover +/- proceed.
For invasive treatment options like surgery, informed consent must be sought from the patient or their relatives for that treatment, these range from consent forms (Consent 1) which is used for individual patients who are deemed to have the capacity, to make an informed decision about their own care. To consent forms (Consent 4) which considers patients who need support with their care and requires a legal caregiver to make those decisions. (NHS, 2022)
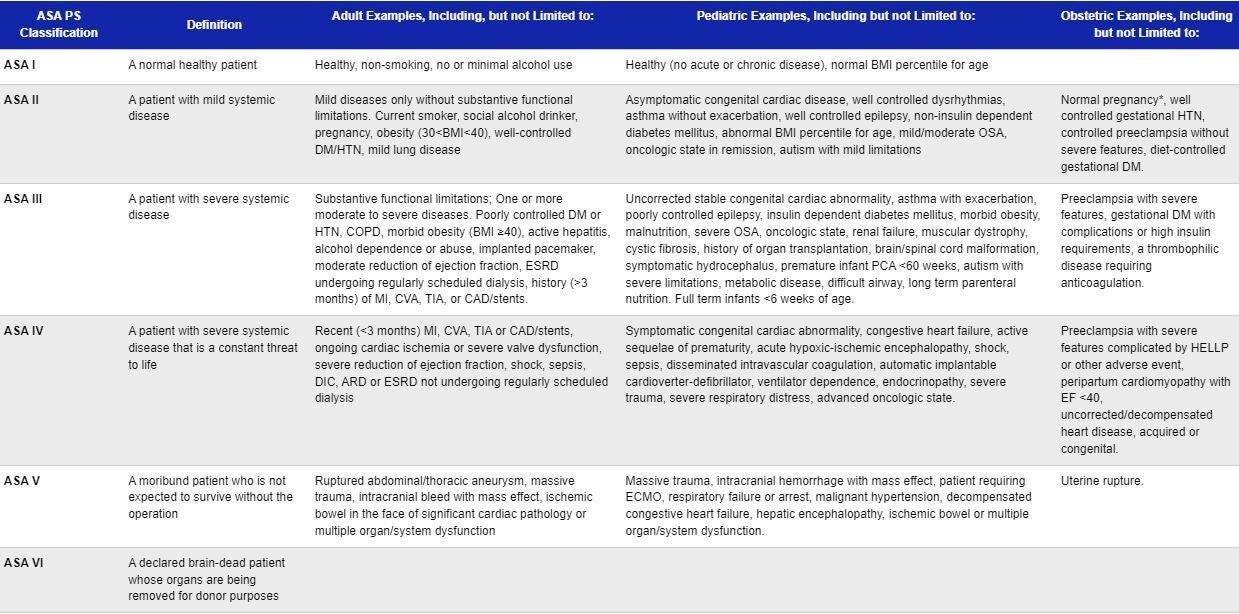
ASA Grading:
A common term within the perioperative field ASA (American Society of Anaesthesiologists) grading is used to give indications on the physical condition of any given patient. Developed in the 1940s to give clinicians a gauge of the risk being undertaken for each patient they encounter. (Kannan, 2017)
The system is graded from 1 to 6, with ASA 1 patients being fit and well and ASA 6 patients being declared brain dead and are donating their organs.
For this surgery Georges ASA grade is ASA 3, this is due to his severe systemic peripheral vascular disease, Smoking and consumption of Alcohol.
American Society of anaesthesiologists, (2020)
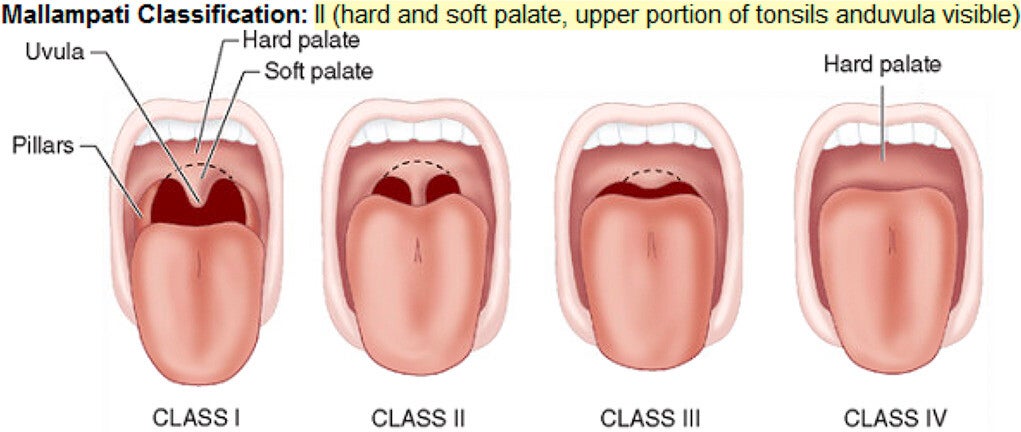
Mallampati Scpre:
Mallampati scoring is used to evaluate a patient's airway for any potential difficulties that may be encountered when attempting intubation. This can be influenced by width of the mouth opening and the view of the soft pallet and other structures within the mouth. (Stutz and Rondeau, 2023)
Additionally incorporated into this Airway assessment is a examination of the patients neck, neck movement and anything else that may interfere and create a difficult airway. (Crawly and Dolton, 2014)
George has a Airway grade of 2 meaning there is a obstructed view of the soft pellet, he also has good neck movement.
Green and Roback, (2019)
Cell Salvage and Group and Save:
The use of cell salvage was recommended for George's procedure, this was recommended due to the nature of the surgery George is to undergo, as there is a higher risk of blood loss as the surgeons will be operating on major blood vessels including the Aorta.
This recommendation is in line with guidance produced by Klein et al, (2018) which recommends that cell salvage should be used if blood loss is predicted to surpass 500ml. Additionally Klein et al, (2018) found that for open aortic surgery the use of cell salvage reduced the transfusion of red cells by 37%.
It is essential that George has a sample of his blood sent to the lab for a ‘group and save’ this allows for his blood group to be identified and any antigens detected so the appropriate blood can be dispensed if George requires any further blood product transfusions peri and post op. Norfolk, (2013)
High Dependency Bed:
During both the pre-op clinic and anaesthetic assessment, it was identified that due to the invasive nature of the surgery, George may benefit from a high dependency bed on the intensive care unit. This post operative care is common in open aortic surgery as shown by Duncan and Pichel, (2022) it also allows for the option to be supported by mechanical ventilation if necessary.
Create Your Own Website With Webador